

The average Australian visits a community pharmacy. 18 times a year – More than another health service.
Pharmacies will only gain more importance as Australia’s population gets older and sicker, and more scripts are disbursed.
But policy failures are holding the sector back. Personal interests govern decision-making. Prices and services are usually not evidence-based. And regulations stifle competition, innovation and discounting.
A brand new Grattan Institute Report Shows how one can shape the pharmacy sector for the long run.
Secret backroom deals
Australian pharmacy policy is a case study in bed governance.

Pharmacies are funded and controlled by Community pharmacy contracts Discussions between the Federal Government and the Pharmacy Guild of Australia took place.
The Guild represents most Australian pharmacy owners. It is some of the powerful political lobby groups within the country. Over the past five years, it has donated A$2.5 million to political parties, making it the biggest donor from the health care sector.
No other Australian health industry group negotiates its funding behind closed doors, without public evidence to justify decisions. These opaque negotiations have to be replaced by free, transparent, evidence-based policy decisions.
Looks like we’re paying an excessive amount of.
When a pharmacy dispenses a Pharmaceutical Benefit Scheme (PBS) medicine, it receives The fee To cover labour, administration and handling. The patient pays as much as the utmost co-payment, and the federal government pays the remaining.
As with much in pharmacy policy, shelling out fees are set by negotiation with the guild, with no public data to justify the numbers. As a result, we won’t know if the value is correct – but there are signs that it’s too high.
Per-script funding has increased whilst e-prescriptions and automation have reduced the labor involved in shelling out. The guild’s own Data suggest that member profits have greater than doubled in real terms over the past decade.
Source: PBS (2017–2025), CC BY-NC-SA
The accuracy is clear. Government funds mustn’t be discussed in any respect. As with public hospitals and aged care, this ought to be determined by the Independent Health and Aged Care Pricing Authority, based on actual cost data.
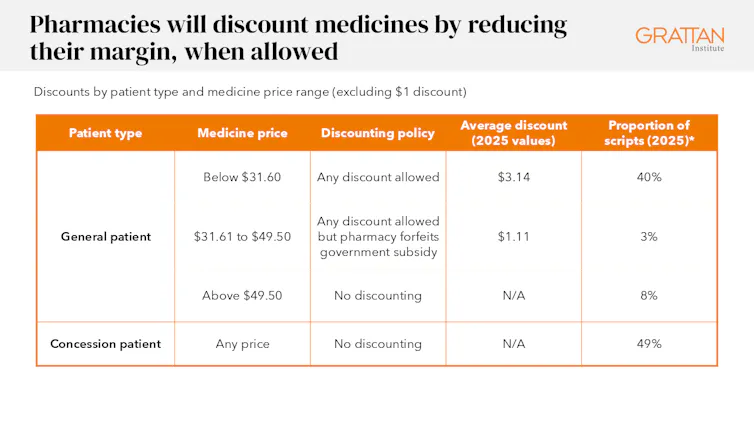
For patients, discounts on PBS drugs are limited by complex rules. These rules rely on how much a drug costs overall, counting funding from each patients and the federal government.
For most cost-effective medicines, discounts are allowed. For the most costly, it is totally banned. For those in the center, pharmacies may offer a reduction, but provided that they offer up all of their government funding for the script.
In 2015, an optional $1 discount on maximum patient out-of-pocket was introduced, but is being phased out. It ought to be restored and increased over time.
something claim It is unfair if some patients get discounts while others don’t. People in areas with less competition between pharmacies usually tend to miss out. But these are usually not surcharges — total fees are capped — and discounts at one pharmacy don’t come on the expense of patients at one other pharmacy.
Even if there ought to be a restriction on shelling out, the foundations we’ve, which prevent discounts for some drugs and never others, make little sense.
Department of Health, Disability and Aging Grattan Analysis (2026), CC BY-NC-SA
Services ought to be well priced.
Proposals to expand the services that pharmacies can offer — including things like prescribing and chronic disease management — have sparked heated debate.
Guilds and pharmacist workforce groups to say More pharmacy services are a commonsense solution to the growing demand for primary health care. But medical institutions to warn This would fragment care and jeopardize patient safety.
Evidence suggests it isn’t so black and white.
International Studies Show pharmacists can safely provide quite a lot of services, including prescriptions, and that these services are popular with patients.
But with rapidly increasing healthcare demand and costs, services must also offer good value for money. The evidence here could be very weak. This is because pharmacies pose unique risks to value.
Walk-in appointments mean some conditions are treated that may resolve on their very own. There is a risk of duplicating GP care. And the retail setting creates business incentives to advertise unnecessary care.
Only one recent service is sufficiently cost-effective. Evidence For national rollout: prescribing for uncomplicated urinary tract infections.
International evidence for another services is promising. But dozens Funded by Govt Trials have failed to indicate their cost-effectiveness here.
The federal government should coordinate robust national trials that concentrate on probably the most promising services, similar to treating shingles and prescribing contraceptives.
Get the pharmacist to work with the GP.
It’s time for a brand new type of measurement.”Integrated PharmacistRather than shelling out, they work alongside GPs on the whole practice to supply medication reviews and patient education.
The UK and Canada already largely fund these positions. Australia too, with government funding for pharmacists on the whole practice and Aboriginal Community Controlled Health Organisations.

James Ross/AAP
Keep up the competition
Pharmacies are private businesses that receive billions of dollars in government funding. In turn, they need to face competition that promotes higher efficiency, quality and convenience – identical to other businesses.
But location rules dictate how close a brand new pharmacy can open to an existing pharmacy, and the way far an existing pharmacy can move.
Several European countries lifted similar restrictions within the late Nineties and early 2000s. The result was more pharmacies, longer opening hours, and, in lots of cases, lower prices.
Proprietary laws prohibit anyone but a pharmacist from owning a pharmacy. Pharmacies are presupposed to prioritize patient care. But we don’t apply this principle elsewhere. Standards of care are maintained through clinician training, registration and accountability, no matter who owns the business. Pharmacists already perform these responsibilities.
Together, location and ownership regulations prevent a small group from competing on price or quality.
The government should scrap these rules, and ask the competition watchdog to design competition safeguards together with independent reporting on standards and results.
The pharmacy of the long run
The current community pharmacy contract expires in mid-2029. Three years is sufficient to gather cost data, initiate trials, enact competition reform laws, and establish quality oversight.
If the federal government acts now, the present contract – the eighth – ought to be the last.