
What is massive cell arteritis?
Giant cell arteritis, also referred to as temporal arteritis, is a disease during which the massive arteries and their branches, including those supplying the attention, skull, and face, turn into inflamed and narrow. This disease may cause vision loss, so it is vital to diagnose and treat the issue as soon as possible. Large blood vessels, including the aorta and its branches, can even turn into involved, resulting in weakening and even rupture of the blood vessels years later.
The disorder occurs almost exclusively in people over the age of 55, and typically affects people of their 70s and 80s. It is comparatively rare: in people over the age of 55, it affects an estimated two in 1,000 people.
The explanation for giant cell arteritis is just not known, even though it has been speculated that in some people the body’s immune system responds incorrectly to an infection, and begins to attack the liner of the blood vessels as if it were a foreign invader. There may additionally be a genetic contribution, as suggested by occasional cases that affect multiple member of the identical family. One possibility is that the immune system of certain individuals or members of the family could also be genetically programmed to reply abnormally to infection, a response that leads to massive cell arteritis.
Symptoms of giant cell arteritis
The commonest symptom is a dull, throbbing headache, often on one or either side of the brow, although it may occur anywhere on the highest of the pinnacle or within the neck. Other common symptoms include a number of of the next:
- fever
- Jaw pain after chewing
- Loss of appetite
- Fatigue
- Dry cough
- Tenderness of scalp or temples
- Blurred vision or lack of vision in a single eye
- Pain within the shoulders, upper arms, or upper hips or thighs, especially within the morning (typical of polymyalgia rheumatica, an arthritic condition related to giant cell arthritis).
Diagnosis of giant cell arteritis
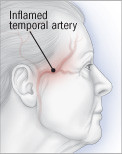
Your doctor may suspect you might have this disorder when you’re an older adult with recent headaches. He will start by asking you for an in depth description of your symptoms, past medical problems, and medications. Next, the doctor will examine you, paying particular attention to your temporal artery, which is positioned above the jaw just in front of the ear, and other blood vessels.

Your doctor will consider other causes of headaches or other symptoms and should order tests to rule out these conditions. However, if giant cell arteritis continues to be a powerful concern after these tests, blood tests to detect inflammation, called erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), could also be ordered because they are often elevated on this condition.
Temporal artery biopsy is normally considered the definitive test to ascertain the diagnosis. In this procedure, a small piece of blood vessel shall be removed under local anesthesia and examined in a laboratory. Other tests, including ultrasound of the temporal arteries, could also be useful in detecting this condition, and in some cases could also be relied upon as a substitute of requiring a biopsy. However, temporal artery ultrasound is just not universally available for this purpose. If temporal artery biopsy and/or ultrasound usually are not diagnostic but concern stays for possible giant cell arteritis, computed tomography angiography (CTA), magnetic resonance angiography (MRA), or positron emission tomography (PET) could also be really helpful to discover giant cell arterioles.
Life expectancy of giant cell arteritis
Giant cell arteritis often lasts for no less than several years. However, improvement often begins inside days of starting therapy. Some persons are in a position to stop treatment inside six months, but longer treatment for 2 to a few years is more common. Occasionally, the disease returns after a protracted period of remission.
Prevention of giant cell arteritis
There isn’t any solution to avoid this disease. Vision loss (and, perhaps, other complications) could be prevented with prompt diagnosis and treatment.
Treatment of giant cell arteritis
Giant cell arteritis is a serious disease that requires immediate medical attention because delay in diagnosis and treatment can result in vision loss or other complications. The essential treatment is high doses of prednisone, a corticosteroid, and most of the people feel higher inside a couple of days. The medication is sustained at high doses for a couple of month after which regularly reduced to the bottom possible dose over the next months, or stopped.
A minimum of six months of treatment is required for individuals with this disorder. Treatment often lasts a 12 months or more because many individuals experience symptoms of polymyalgia rheumatica (pain within the shoulders, hips, or each) or frequent headaches because the prednisone dose is tapered.
In 2017, tocilizumab (Actemra) was approved as an injectable treatment for big cell arteritis because studies showed that, together with corticosteroids, it was effective for the condition, including a steroid-sparing effect. This medication could also be really helpful if symptoms return repeatedly as steroids are tapered off, or if there are other conditions for which steroid therapy could also be particularly troublesome (including diabetes or osteoporosis).
In 2025, upadacitinib (Rinvoq) was also approved for the treatment of adults with giant cell arteriosclerosis. This oral medication could also be prescribed for individuals with giant cell arteritis based on personal preference, cost, convenience, or specific concerns about unintended effects of other treatment options.
Some studies have found that one other drug, methotrexate (Folex, Rheumatrix), can reduce the dose of corticosteroids needed and the time needed to take them, although other studies haven’t confirmed this. As a result, some physicians prescribe methotrexate as a “steroid-sparing” agent in hopes of reducing overall exposure to corticosteroids. However, evidence to this point suggests that tocilizumab is more practical than methotrexate as a steroid-sparing drug.
Steroid use can result in complications including osteoporosis, diabetes, and weight gain. Measures to stop these complications (equivalent to extra calcium and vitamin D) are routinely really helpful. Bone densitometry testing can also be really helpful to observe bone density and detect osteoporosis. Research is ongoing to discover other effective steroid sparing drugs.
Some research suggests that low-dose aspirin may help prevent complications of giant cell arteriosclerosis, including vision loss. Although the actual effectiveness of aspirin is uncertain, it could be really helpful together with steroid therapy for this condition.
When to Call a Professional
If you might have symptoms of giant cell arteritis, especially a brand new headache, unexplained fever, or visual symptoms, it’s best to contact your doctor.
Assessment
If vision is just not affected, vision is great. However, once vision loss occurs, it is normally everlasting. If the aorta or its surrounding branches are involved, the prognosis could also be worse, as these blood vessels may enlarge or rupture. However, most complications related to massive cell arteritis are brought on by steroid therapy quite than the disease itself.
Additional information
American College of Rheumatology
http://www.rheumatology.org/